Background
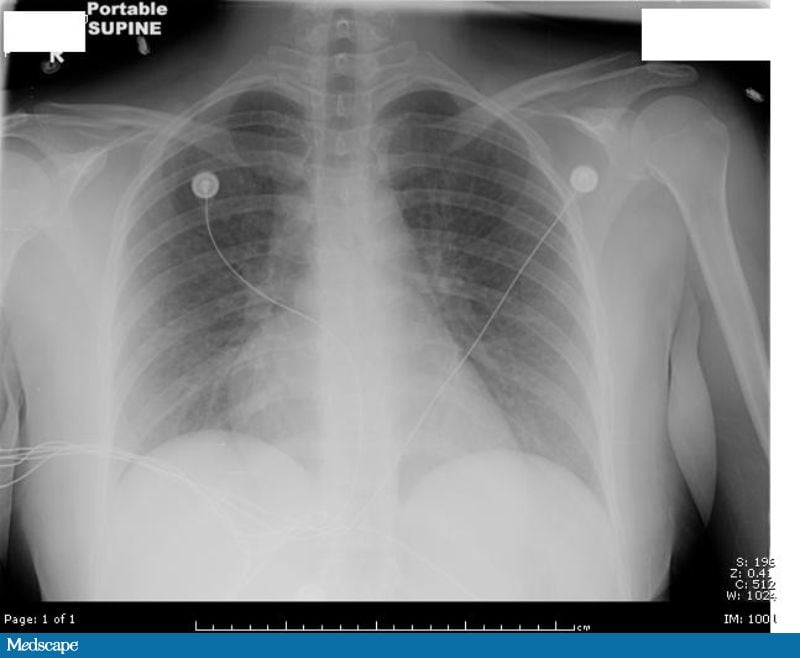 Figure 1. (Click to enlarge) |
A 25-year-old woman presents to the emergency department (ED) with a 2-day history of dull left lower quadrant (LLQ) pain and a diffuse pinkish rash. One week ago, she was diagnosed with streptococcal pharyngitis at an urgent care center for students and was discharged with a prescription for amoxicillin. Three days later, she developed the pinkish rash; the rash was diagnosed by a dermatologist to be an allergic reaction to the amoxicillin. The dermatologist prescribed prednisone and discontinued the amoxicillin. The patient subsequently developed nausea, vomiting, fever, and the aforementioned LLQ pain. She denies experiencing any vaginal bleeding or discharge, dysuria, increased urinary urgency or frequency, melena, or hematochezia. She reports feeling weak and dizzy. Other than her visit to the student urgent health care center, she has no past medical history, is not taking any medications, and does not have any allergies. She does occasionally drink alcohol, but she denies smoking tobacco or using illicit drugs. She also denies using tampons.
On physical examination, she is noted to be alert and have a normal mental status, but is otherwise pale and ill-appearing. Her blood pressure is 65/35 mm Hg, with a regular heart rate ranging between 110-120 bpm. Her respirations are measured at 20 breaths/min, her oral temperature is 103.46°F (39.70°C), and her oxygen saturation is 93% while breathing room air. The integument examination reveals a diffuse, erythematous, blanching rash; however, the integument is otherwise warm and dry to the touch. The oropharynx is clear, with no exudates or erythema. Diffuse mild crackles are noted in the patient's lungs. She has normal heart sounds, with a regular rhythm and a slightly increased capillary refill. Her abdomen is soft and minimally tender to deep palpation in the LLQ. No abdominal masses or hepatosplenomegaly are appreciated. The pelvic examination reveals no external vaginal or cervical lesions, cervical motion tenderness, or adnexal masses or tenderness. No foreign bodies are visualized.
The laboratory examination, including a complete blood cell (CBC) count and comprehensive metabolic panel, is essentially unremarkable, except for a white blood cell (WBC) count of 31.6 × 103/µL (31.6 × 109/L), band neutrophils of 13% (0.13) and a creatinine of 2.4 mg/dL (212.16 µmol/L). Her arterial blood gas analysis is remarkable for a partial pressure of carbon dioxide (pCO2) of 27 mm Hg (3.59 kPa), a partial pressure of oxygen (pO2) of 56 mm Hg (7.45 kPa), a bicarbonate of 19 mEq/L (19 mmol/L), and a base deficit of 4.4 mmol/L (normal range, 0-2 mmol/L). The urinalysis, cervical Gram stain, and potassium hydroxide (KOH) wet preparation are all normal. A chest radiograph is taken that shows changes consistent with early adult respiratory distress syndrome (ARDS; see Figure 1).
Upon returning from the radiology department, she is noted to again become hypotensive, tachycardic, and tachypneic, as well as remaining febrile despite the administration of acetaminophen. An elective rapid-sequence intubation is performed for the pending respiratory failure. She is diagnosed with septic shock (etiology unknown) and treated empirically with clindamycin, vancomycin, and meropenem. Blood, urine, and respiratory cultures are obtained, and antistreptolysin O (ASO) and toxic shock syndrome toxin–1 (TSST-1) antibody titers are ordered. A lumbar puncture is deferred, and the patient is admitted to the medical intensive care unit (ICU).
Discussion
| Figure 1. (Click to enlarge) | 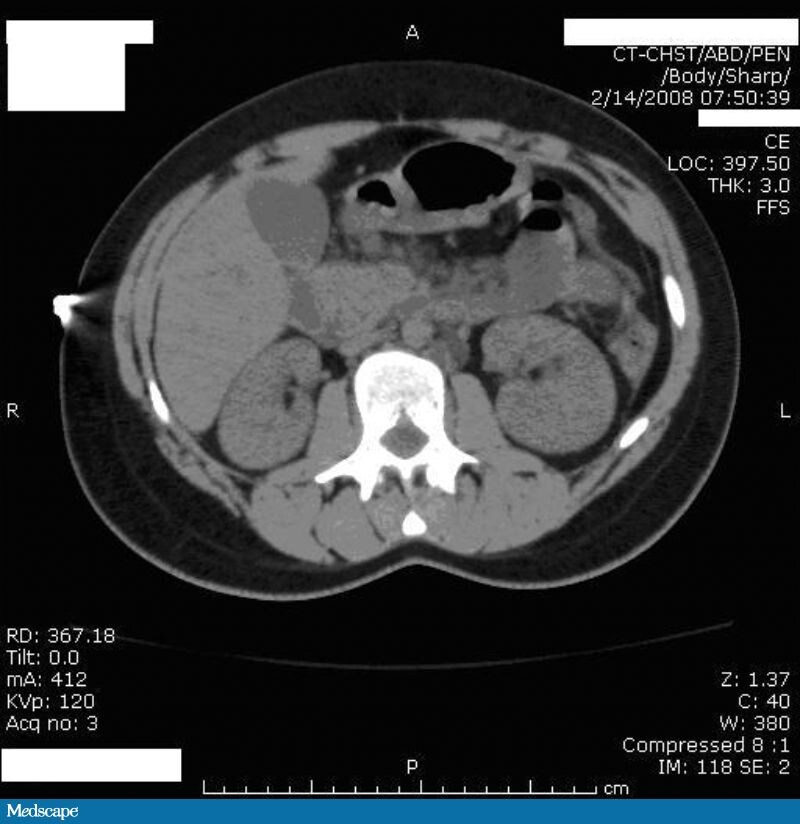 Figure 2. (Click to enlarge) |
Toxic shock syndrome (TSS), mediated by enterotoxins produced by Staphylococcus aureus or Streptococcus pyogenes, became prevalent in the early 1980s (for S aureus) and 1993 (for S pyogenes). Staphylococcal TSS was first described in 1978, when 7 children presented to an emergency department with acute-onset fever, vomiting, diarrhea, and sore throat; they subsequently went into septic shock and multiorgan dysfunction.[1] In the early 1980s, the incidence of staphylococcal TSS among healthy, young, menstruating women increased. Eventually, it was discovered that a specific manufacturing defect in tampons linked staphylococcal TSS to their use. The tampons were believed to neutralize the acidic vaginal environment during menstruation, thus promoting oxygen tension and raising carbon dioxide levels in the vagina, providing a proper medium for the growth of S aureus. Once the link was discovered, the manufacturing of tampons was changed, and the overall incidence of S aureus TSS declined from 12 cases per 100,000 population in 1980 to 1 case per 100,000 population in 1986. The reported incidence, as of 1996, is at 0.5 cases per 100,000 population.[2,3]
Group A streptococcal TSS was not well described until 1993, when children who had suffered from varicella presented roughly 2-4 weeks later with a clinical syndrome highly suggestive of staphylococcal TSS. The incidence rate was shown to be between 4.3 and 5.5 cases per 100,000 population in 1999, with a mortality rate of about 5-10% in children and 30-80% in adults.[3] In 1993, the following consensus definition for streptococcal TSS was created[4]:
- Isolation of group A Streptococcus from a normally sterile site (ie, blood, cerebrospinal fluid, pleural or peritoneal fluid)
- Hypotension
- Two or more of the following:
- Renal impairment (a creatinine >2.0 mg/dL [176.8 µmol/L] or 2 times the baseline value for a patient with renal disease)
- Coagulopathy
- Elevated liver enzyme tests
- Adult respiratory distress syndrome (ARDS)
- Erythematous macular rash
- Soft tissue necrosis
The pathophysiologic connection between varicella and streptococcal TSS has yet to be determined, but the introduction of the vaccine substantially decreased the incidence rate, from 27% during the prevaccination period in 1993-1995 to 2% in 1999-2001 (at which time use of the vaccine had become widespread). As a result, Stevens et al postulated that there is a link between a manifestation of the herpes zoster virus and the incidence of TSS. The actual correlation between the 2 entities has yet to be fully deciphered.[2] Interestingly enough, nonsteroidal anti-inflammatory drug (NSAID) use has also been shown to be a risk factor for both types of TSS. A review article by Chuang et al in 2005 described a 1992 study in the UK showing that 92% of patients with TSS had previous NSAID use. This study reported that NSAIDs are believed to mediate TSS development, as they impair granulocyte function while enhancing the production of cytokines. As such, NSAIDs can mask disease progression and delay the diagnosis by relieving pain, reducing swelling, and suppressing fever.[3]
Patients with either type of TSS often present with fever, rapid-onset hypotension, and generalized malaise following nonspecific prodromal symptoms. Subsequently, these patients will quickly develop multisystem organ dysfunction, including acute renal failure, ARDS, and disseminated intravascular coagulation (DIC). The serum creatinine will be elevated to at least 2.0 mg/dL (176.8 µmol/L; or, at least twice the baseline value for a patient with established renal disease) and, in 40-50% of patients, it often precedes hypotension. Furthermore, in 55% of patients, ARDS also precedes hypotension, presenting as hypoxia and tachypnea.[5]
Differentiating between staphylococcal and streptococcal TSS is often difficult at the initial presentation. As noted above, these syndromes usually present with nonspecific constitutional symptoms and generalized signs. The focality of infection is often the nasopharynx, oropharynx, vagina, or skin; however, in about 50% of cases, there is no identifiable focus. On the other hand, there appears to be some symptoms and signs that may assist in distinguishing between the 2 etiologies. Patients with staphylococcal TSS tend to present with diarrhea, vomiting, generalized erythroderma, conjunctival injection, and/or severe myalgia. Patients with streptococcal TSS, however, often have a form of soft tissue necrosis (eg, cellulitis, abscess, myositis, or necrotizing fasciitis), influenza-like symptoms, and (as previously described) varicella in those patients who have not been vaccinated against it.[1]
Laboratory tests are often the only way to distinguish between the 2 etiologies. As previously mentioned, both types of TSS are mediated by enterotoxins. In staphylococcal TSS, toxic shock syndrome toxin–1 (TSST-1) is responsible for nearly 75% of cases; it has been found in 90% of menstrual cases and 50-60% in nonmenstrual cases. Testing for this toxin involves detecting the presence of antibodies against it. If TSST-1 antibodies are present in the laboratory studies, the specificity of TSS being caused by S aureus is up to 90%. S pyogenes TSS, on the other hand, is mediated by different enterotoxins, but all are linked to the M-protein found in the cell membrane of the bacterium. Streptococcal pyrogenic exotoxins (SPEs) A, B, and C are present in only about 13% of S pyogenes–mediated TSS-related cases; however, laboratory testing suggests that the M-protein is present in about 75% of these cases. Unfortunately, no reliable tests detecting M-protein exist at this time. Streptolysin O, however, is another toxic immunogenic protein produced by S pyogenes. Its presence during an infection can be measured using the titer against antistreptolysin antibody (ASO titer). The sensitivity of this test ranges from 62-76%, with a specificity of 79-85%; therefore, elevated titer levels will often identify S pyogenes as the etiologic bacterium. Lastly, blood cultures will be positive in about 75% of cases of streptococcal TSS; however, with staphylococcal TSS, 50% of blood cultures are positive in cases of nonmenstrual TSS, whereas less than 5% result positive in menstrual TSS cases.[3,6,8]
Regardless of the bacteria causing TSS, the treatment remains the same. Crystalloids and inotropic agents are used to aggressively treat the hypovolemic shock, with close monitoring of the patient's mean arterial pressure (MAP) and central venous pressure (CVP). Furthermore, targeted antibiotics are indicated; penicillin or a beta-lactam antibiotic is used for treating group A streptococci, and vancomycin or a semisynthetic antistaphylococcal penicillin is used for staphylococcal TSS. Clindamycin, however, has emerged as a key portion of the standard treatment. When utilized, clindamycin has an 83% more favorable outcome when compared with penicillin or beta-lactam antibiotics (14%).[3] As opposed to penicillin, clindamycin is not affected by the size of the inoculum, it has a longer postantibiotic effect, and it better facilitates phagocytosis by inhibiting the production of the antiphagocytic M-protein. In addition, clindamycin reduces TSST-1 levels by up to 90%, whereas penicillin or other beta-lactam antibiotics have the potential to raise TSST-1 levels because they will lyse or alter the bacterial cell membrane, which often causes further release of the toxin into the bloodstream. The use of other adjunctive therapies, such as intravenous immunoglobulin (IVIG), hyperbaric oxygen, and anti–tumor necrosis factor (TNF) antibodies, is still in the research phases at this time.[3,7] The role of activated protein C is still unproven.
The respiratory status of the patient in this case was noted to steadily improve after admission to the ICU, and the patient was extubated 48 hours later. She was continued on clindamycin and meropenem. A lumbar puncture was performed 4 hours after her initial presentation, and a second puncture was performed approximately 1-2 hours after antibiotics were started. The results of the lumbar puncture showed normal glucose and protein levels, with no white blood cells, a negative Gram stain, and negative cultures. Her human immunodeficiency virus (HIV), influenza A/B antigens, Coccidioides immitis, and infectious mononucleosis cultures were all negative, as were her blood, urine, and respiratory cultures. The TSST-1 antibody titer returned 2 weeks later as positive, while her ASO titer was normal. She was eventually switched to oral antibiotics, and her renal function and WBC count slowly normalized. Daily chest radiographs showed that her ARDS was resolving. She was discharged to home 14 days after her initial presentation. The patient's final discharge diagnosis was staphylococcal TSS stemming from a probable respiratory illness (such as pneumonia).
e. Penicillin plus vancomycin plus gentamycin
d. Staphilococal skin syndrome

No comments:
Post a Comment